Advanced Terminology Mapping Examples
In the previous What is Mapping in Terminology blog article, we introduced key mapping characteristics. We go further in this article by providing examples of those characteristics in addition to introducing a few more advanced topics.
Visit our product page for more information on West Coast Informatics open source mapping tool.
When to Create a Simple Map vs. a Complex Map?
Simple maps are used for map sets in which source codes are mapped to exactly zero or one target codes without additional rule-based logic. When map sets require rule-based predicate logic or differences in terminology granularity require a source code to be mapped to more than one target code, then Complex Maps are used.
Most map sets that make use of simple maps are designed to represent equivalence or near-equivalence between source and target codes in the respective terminologies.
Typically, each simple map will express the nature of the one-to-one relationship between source and target code as equivalent, broader, or narrower. The most common other situation is the One-to-None case, where the source code does not have a corresponding code in the target terminology.
One-to-One - In the One-to-One mapping example below, the source SNOMED CT concept “Pleomorphic lobular carcinoma” is mapped to a broader target ICD-O target code of 8520/3 “Lobular carcinoma, NOS”.
One-to-None - In the One-to-None mapping example below, the source SNOMED CT concept “Corneal epithelial map lines” does not have a mapping to an ICD-10 target code as this is a clinical finding that has no effective representation in ICD-10.

Must all Source Concepts be Mapped?
No. When creating maps between a source and target terminology, scope definitions are used to define which codes are to be mapped and which codes are allowed to be mapped to.
For example, the SNOMED CT- to-ICD-10 map only considers SNOMED CT concepts in the “clinical finding”, “situation”, and ”event” hierarchies to be mappable.
It is also the case that even for codes within the defined scope, there is no valid choice for a map. For example, the source SNOMED CT concept “Corneal epithelial map lines” does not have a mapping to an ICD-10 target code as this is a clinical finding that has no effective representation in ICD-10.

Must all Source Concepts have a Map to a Target Concept?
No. For example, the SNOMED CT concept “Corneal epithelial map lines” does not have a mapping to an ICD-10 code as this source concept is a clinical finding that has no effective representation in the target terminology ICD-10.
When Would One Create a Complex Map Rather than a Simple Map?
Complex Maps are used in situations where source codes in a terminology may have multiple relevant codes in the target terminology, or when a rule-based predicate is needed to determine the correct target code(s). When every source code has exactly zero or one appropriate target codes, Simple Maps should be used.
A complex map with a rule-based predicate requires the evaluation of potentially external criteria to arrive at the correct mapping from a source concept to a target terminology.
For example, the age or gender of the patient from the medical record may be needed to determine the correct target code.
When used, rule-based predicates are generally expressed in both human-readable format for manual evaluation as well as machine-readable format for automated evaluation via a rules engine.
What are Some Examples of Complex Mappings?
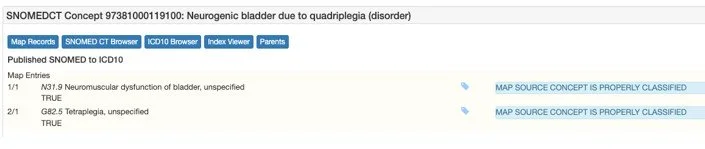
One-to-Many - In the One-to-Many mapping example below, the source SNOMED CT concept “Neurogenic bladder due to quadriplegia” maps to a combination of two target ICD-10 codes: N31.9 “Neuromuscular dysfunction of bladder, unspecified” and G82.5 “Tetraplegia, unspecified”.

One-to-None - In the One-to-None mapping example below, the source SNOMED CT concept “High risk human papillomavirus detected” will result in a No Map in the target terminology if it cannot be determined or it is not recorded whether the patient is male or female.

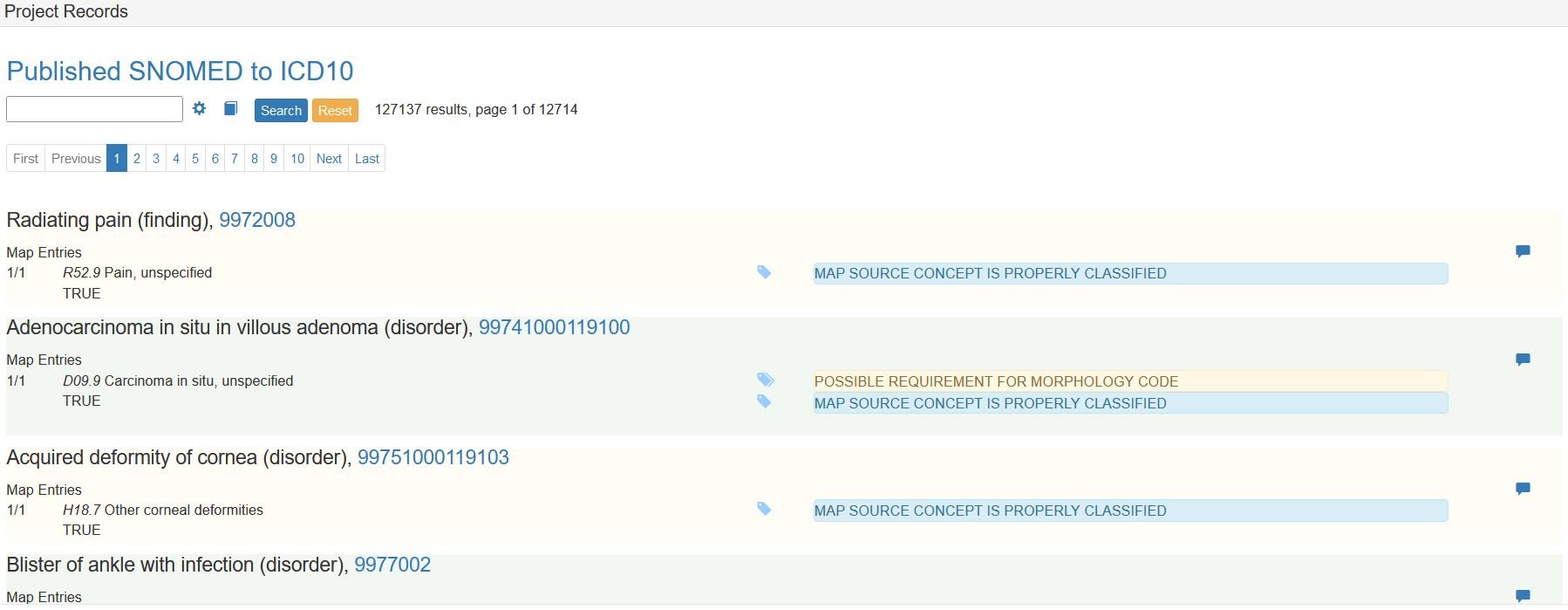
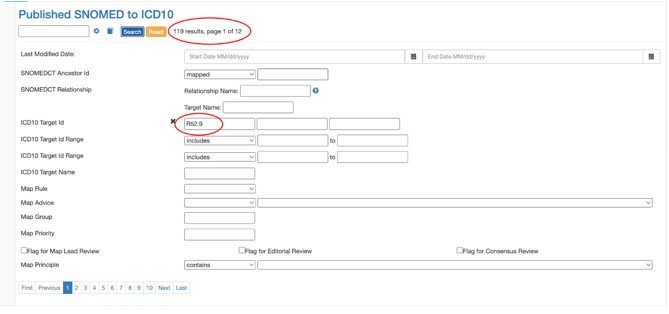
Many-to-One - In the Many-to-One mapping example below, if we search for mappings to a given target code, we can find examples where one target code is mapped to by multiple source codes. In the example below we see the ICD-10 code R52.9 “Pain, unspecified” is the target code in 119 SNOMED CT mappings.

What is an Example of a One-to-One Map?
One-to-One mappings are considered to be simple maps. These do not require the processing of any rules or advice to determine a mapping to a target terminology. The target code for this mapping may or may not be an exact equivalent code.
In the simple mapping example below, the source SNOMED CT concept ”Pleomorphic lobular carcinoma” is mapped to a broader target ICD-O code of 8520/3 ”Lobular carcinoma, NOS”.
What is an Example of a One-to-Many Map?
In the One-to-Many mapping example below, the source SNOMED CT concept “Neurogenic bladder due to quadriplegia” maps to a combination of two target ICD-10 codes: N31.9 “Neuromuscular dysfunction of bladder, unspecified” and G82.5 “Tetraplegia, unspecified”.
What is an Example of a One-to-None Map?
In the One-to-None mapping example below, the source SNOMED CT concept “High risk human papillomavirus detected” will result in a No Map in the target terminology if it cannot be determined or it is not recorded whether the patient is male or female.

What is an Example of a Many-to-One Map?
In the Many-to-One mapping example below, if we search for mappings to a given target code, we can find examples where one target code is mapped to by multiple source codes. In the example below we see the ICD-10 code R52.9 “Pain, unspecified” is the target code in 119 SNOMED CT mappings.
What is a Map Group?
This is a mechanism defined by the SNOMED CT RF2 Extended Map format that supports the ability to indicate the numerical sequence of target codes in a complex map.
When a single concept in a source terminology maps to multiple codes in the target terminology this type of mapping can be represented in a couple of ways. If there is no need to process advice or rules then you can simply combine the two target codes in a single line in the map using some kind of concatenation character. If the selection of more than one code is dependent on rules then you will need some way to independently validate each rule to arrive at the separate codes.
In the example below, there is a first map group that always points to the target code H90.5. In the second map group, there are two possible target codes depending on the evaluation of a rule-based predicate - whether the patient is Male.

What is an Example of a Map Group?
In the example below, there is a first map group that always points to the target code H90.5. In the second map group, there are two possible target codes depending on the evaluation of a rule-based predicate - whether the patient is Male.
What is a Map Priority?
This is a mechanism defined by the SNOMED CT RF2 Extended Map format that is used to sequence entries in a map when rule-based predicates are used. Logic is applied in a particular order in order to determine the appropriate map target.
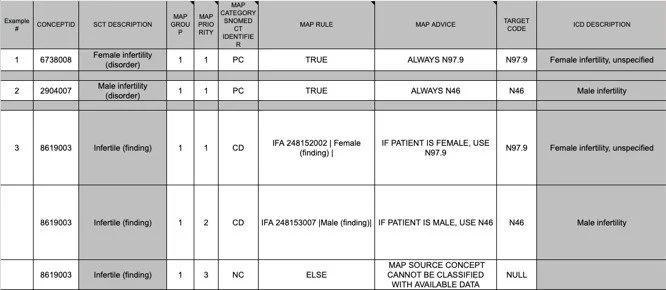
Map priority is used to evaluate criteria in a specific order. In the example below from the SNOMED CT to ICD-10 Examples, source concept for “Infertile” has a different mapping depending whether the patient is female, male, or not known. The priority indicates that when processing this map, it should be first checked whether the patient is known to be Female, then checked whether the patient is known to be Male, and otherwise a third target code is to be used.
What is an Example of Map Priority?
In the map priority example below from the SNOMED CT to ICD-10 Examples, source concept for “Infertile” has a different mapping depending whether the patient is female, male, or not known. The priority indicates that when processing this map, it should be first checked whether the patient is known to be Female, then checked whether the patient is known to be Male, and otherwise a third target code is to be used.
What is a Mapping Rule?
Mapping Rules are rule-based predicate logic meant to be evaluated by a computer to determine which of a variety of potential target codes should be used for the given situation.
See the National Library of Medicine (NLM) I-Magic tool for an example of an implementation of the rules expressed in the SNOMED CT to ICD-10-CM map.
What is a Map Advice?
Map Advice is additional structured information about how to use a particular map entry. It may require or suggest the use of an additional code for extra context about a particular medical situation, or it may refer to underlying mapping guidance published elsewhere, or may simply provide additional information about source or target codes.
In the example below from the SNOMED-to-ICD-10 Map Examples you see the Map Advice specifying the possible requirement for a place of occurrence.

What is an Example of Map Advice?
In the example below from the SNOMED-to-ICD-10 Map Examples you see the Map Advice specifying the possible requirement for a place of occurrence.
How are Mapping Rules Formatted?
Since source and target terminologies represent information in different ways, there is no single standard format for representing map rules. Typically, maps produced by a given organization will have a structured approach to map rules. For example, mapping rule grammar and formatting used for the SNOMED-to-ICD-10 mapping can be found here.
Why is Mapping Direction Important?
Mappings are directional and created from one terminology (the source) to another terminology (the target). While there may be some cases where the target code for a particular source code is an exact match, that does not imply no other source codes would map to the same target code. For example, in the SNOMED CT-to-ICD-10 mapping the concept 9972008: ”Radiating pain (finding)” maps directly to R52.9 ”Pain, unspecified”. This could be considered an equivalent map.

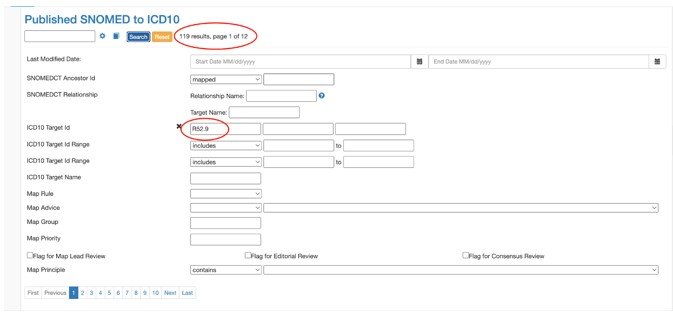
However, if we look at the reverse, R52.9 maps to 119 total SNOMED CT concepts.
Why is an Example where the Mapping Direction in One Direction is Different than the Other?
An example can be found in the SNOMED CT-to-ICD-10 mapping the concept 9972008: ”Radiating pain (finding)” maps directly to R52.9 ”Pain, unspecified”. This could be considered an equivalent map.
However, if we look at the reverse, R52.9 maps to 119 total SNOMED CT concepts.
What is an Example of a Bi-Directional Mapping Project?
MedDRA has undertaken a project with SNOMED to create a bi-directional map. One can learn more about this mapping project via the SNOMED Confulence Page.
In this case, Each directional map is independent. That is, the SNOMED-to-MedDRA is a different mapping project than the MedDRA-to-SNOMED mapping project.
What is an Example of a Bi-Directional Map?
Consider the following case:
MedDRA-to-SNOMED: MedDRA Concept Emotional lability maps maps to SNOMED CT concept Mood swings (finding)
Yet, when looking at the SNOMED Concept, it does not map to the same MedDRA concept.
SNOMED-to-MedDRA: SNOMED Concept Mood swings (finding) maps to MedDRA concept Mood swings
Questions, ideas or concerns regarding your mapping capabilities? Contact us today and we are available to help your organization.